
Introduction
Project Title: Addressing Mental Health During COVID-19
The idea of this project was initiated in collaboration with my academic advisor. The sponsors associated with this project are my field supervisor and the director of the Lighthouse. The Lighthouse is operated by Helen Ross McNabb Center and offers a peer support program. The program is designed to provide adults with a mental illness to develop social skills in a community setting while receiving support from each other and therefore receiving higher levels of care and personal development. The duration of my project took place over the course of a two-month period. Participants were McNabb Center group home residents who have been diagnosed with mental illness. Because of COVID-19, attendance at the Lighthouse was limited and significantly impacted. Participants in the community settings outside of McNabb Center group homes were no longer allowed to attend the Lighthouse. During my field practice, I conducted a Survey that allowed me to gather data to assess current activities delivered at The Lighthouse and the need for other activities to be integrated into a curriculum focused on the recovery of mental illness. Since attendance and participation in activities decreased, I created and implemented a curriculum focused on recovering from mental illness.
Addressing the Issue and why it matters.
The Issue
The social issues being addressed are decreased attendance and a lack of participation in Lighthouse activities’ regular participants. Interacting with peers and feeling supported, especially during COVID-19, is paramount in preventing suicide, preventing substance use, and other destructive behaviors related to a mental health diagnosis. Due to social distancing and many organizations being closed during the Pandemic, being connected and feeling supported by others has been challenging. Being connected and feeling supported is a key component in managing mental health symptoms (Colorado Department of Education, 2020).
Significance, Implications, and People Affected
This year has had record-breaking impacts on millions of Americans nationwide. The COVID-19 Pandemic brought many changes to how we live our lives and, along with it, uneasiness and uncertainty, altered daily routines, and social isolation. We now may worry about getting sick, how long the pandemic will last, and what the future will bring. Information overload, rumors, and misinformation can make your life feel out of control and make it unclear what to do.
During the COVID-19 Pandemic, persons may experience stress, anxiety, fear, sadness, and loneliness. Mental health disorders, including anxiety and depression, can worsen (Mayo Clinic, 2020). In addition to the fear of contracting the Coronavirus are significant changes to our daily lives as our movements are restricted in support of efforts to contain and slow down the virus’s spread. This is especially true for members in community group home settings, where they are no longer to go on outings to Wal-Mart, the zoo, or other fun-filled activities that they were able to do before COVID-19. At the beginning of COVID-19, the Lighthouse closed to all participants for three-months. Before COVID-19, attendance ranged anywhere from 20-60 people participating in daily activities six days per week to limiting the number of participants to no more than eight, having only two groups per day, one in the morning and the other in the afternoon, to decreasing activities to four-five days per week. Another significant contribution to the community group home members impacted by COVID-19 was that the Lighthouse would have cookouts for holidays and hot meals each Thursday and serve tea daily. This has now been reduced to the Lighthouse director preparing a meal the day before a holiday and delivering it to each group home the next day. The hot meals are now sacked lunches prepared the day before, and only canned sodas are being offered at the end of the group activities for members to take home. The issue is significant in that the peer support center is designed to offer supportive services to help participants learn social skills, provide them with the opportunity for peer interactions, and serve as a means of self-care.
Design of interventions
Mission: To provide support through a curriculum that focused on recovery and address mental health issues associated with COVID-19.
Goals: This project’s primary goal was to increase attendance and address gaps in services that had been lacking based on feedback from participants.
Intervention Tools: The type of interventions used for the peer support groups at the Lighthouse I created for the curriculum were mezzo-level social work practice models. Participants attending the Lighthouse were considered household groups because they lived together in the same group home and peer groups. After all, the participants all had similar problems they were dealing with.
Specific interventions created for use within the curriculum were designed to impact a micro-level of social work practice by teaching skills that would impact the ability to function within the group homes and the community.
The following are links to handouts and interventions that took place throughout the curriculum.
Decision-Making Tree, Symptoms & Recognition of Stress and Stress Management Strategies
Social Support, Values Discussion, and Self-Care Tips and Activities
Deep Breathing Exercises and Sleep Hygiene Discussion
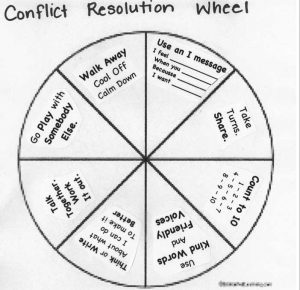
Fair Fighting Rules & Conflict Resolution Wheel
Theoretical Perspectives
Systems Theory – Systems theory in social work is based on the idea that behavior is influenced by various factors that work together as a system. In this project, the system I worked with was clients who reside in group homes in a peer support setting. I observed and analyzed participants within their group home setting, individual therapy settings, and peer support groups. Based on my observations and through data collection from administering surveys, I was able to work to improve behavior and welfare for constituents on a micro and mezzo level of systems. Each intervention focused on improving an individual’s ability to function within their group home setting and functioning within the community.
Psychodynamic Theory – This theory examines the emotional and internal forces that shape human behavior. Interventions used to examine the emotional and internal forces for participants’ behavior were conflict resolution, fair fighting skills, mindfulness, grounding techniques, exploring emotions, and feeling these emotions on our bodies, strengths exploration, and Cognitive Behavioral Theory and Therapy techniques. Please see examples of this theory.
Social Learning Theory – In this theory, one seeks to understand human behavior in how we learn from observing and interacting with others around us. In this project, I worked with adults with mental illness. These adults observed, copied, and modeled behaviors they were taught during the group sessions in which my curriculum was presented. According to the theory’s originator, Albert Bandura, the degree to which such modeling takes place depends on attention, retention, reproduction, and motivation. Participants of this project’s curriculum were able to reproduce behavioral skills taught to them during group time.
Conflict Theory – This theory explains that human behavior can be explained in competition between groups with unequal power. I was able to observe numerous power struggles among participants residing in the McNabb Center group homes. I utilized conflict theory by addressing asymmetrical power relationships between group members. Interventions were created and implemented to reduce tensions among different group members in their group home settings. Interventions included: Anger Management Skills, Conflict Resolution, Stress Management, and Fair Fighting Rules. Conflict Theory intervention examples
Review of Literature
I reviewed the curriculum at the Lighthouse that was being used before implementing my curriculum. The curriculum utilized by the Lighthouse included Wellness Recovery Action Plan (WRAP), Chronic Disease Self-Management Program (CDSMP), and Diabetes Self-Management Program (DSMP). Participants in WRAP reported significant increases in 1) their hopefulness for their own recovery; 2) awareness of their own early warning signs of decompensation; 3) use of wellness tools in their daily routine; 4) awareness of their own symptom triggers; 5) having a crisis plan in place; 6) having a plan for dealing with symptoms; 7) having a social support system, and 8) ability to take responsibility for their own wellness (Cook et al., 2010). Given the rapid growth of this intervention in the U.S. and internationally, these results contribute to the evidence base for peer-led services (Cook et al., 2010). The study results discussed by (Fukui et al., 2014) offer promising evidence that WRAP participation positively affects psychiatric symptoms and feelings of hopefulness. CDSMP results in significant, measurable improvements in patient outcomes and quality of life (Evidence-Based Healthy Aging Program, 2020). Over time, with greater use and research, peer support services can help mental health services fulfill the promise of recovery for those with serious mental illnesses (Chinman et al., 2014). Research findings indicated that the self-management curriculum focused on recovering from mental illness works for this population and is the best curriculum available for this population. WRAP has been rigorously studied and has been proven to work well for people with all kinds of issues and circumstances, including people who have serious mental health challenges and other major life issues (Advocates for Human Potential, Inc., 2018). Topics and activities that were implemented in my curriculum were made to implement WRAP and CDSMP guidelines.
Results Achieved
The implementation of my curriculum increased attendance from 0-5 people per day to 8-18 people per day. This was a significant increase in participants. Before COVID-19, attendance was 20-60 per day. COVID-19 played a dramatic role in the decrease in attendance since the Lighthouse had been closed for three months. I conducted pre and post-tests via surveys to gauge the curriculum’s effectiveness before the creation of my curriculum and to measure the effectiveness of my special project’s curriculum. Pre-Test Survey and Post-Test Survey
Conclusions
There were limitations in implementing the curriculum over a six-week time frame, as I had originally planned for. These limitations involved not being allowed to create a curriculum for any Thursday, Friday, and two Tuesdays per month. The director’s reasoning behind this was because on two Tuesday’s per month, they had an established Nutrition curriculum which they used, and on Thursdays, they had to play Bingo and get a sack lunch; on Friday’s they leave that day for a ‘fun’ day to either watch a movie or sing karaoke. Instead of creating six weeks of the curriculum in a row, I created activities over September and October to work around these limitations.
Another limitation was COVID-19. Due to the Pandemic, community group homes and members were not allowed to attend. This significantly limited the number of participants to McNabb Center group home residents only, and not every resident from the McNabb Center homes attended due to fears related to COVID-19.
Time was also a significant factor in the implementation of the curriculum. I was faced with completing my entire portfolio a month earlier than expected. Therefore, I had to create and implement activities by creating instructions in advance until the end of October for the current peer support staff to review during each group.
When creating the curriculum, I had to plan activities that were not too complex and understood at a lower cognitive ability level. This was due to the varying severity of cognitive functioning for each participant. Even though I created activities that I thought could be understood by the slowest member of the group, some participants still had difficulty understanding. I had to plan to explain in a way each group could understand better. Even though I was not there every day to administer the curriculum, a discussion was made between myself and the peer support staff concerning feedback received and any recommendations I might have.
My Special Project demonstrated all nine of the competencies required by the CSWE.
Competency 1: Demonstrate ethical and professional behavior.
- I made ethical decisions by applying the standards set forth by the NASW Code of Ethics while creating this curriculum, by being attentive to relevant rules and guidelines that were set forth to abide by, modeling ethical decision-making by utilizing evidence-based practices while creating the curriculum and discussing the topics I chose for the creation of the curriculum during supervision and with the director of the Lighthouse. I researched to find topics for the curriculum ethically.
• I used reflection and self-regulation to manage personal values and maintain professionalism in settings involving work with clients, staff, and supervision.
• I demonstrated professional demeanor in my behavior and appearance and oral, written, and electronic communication with clients and staff.
• I used supervision to consult and discuss this special project along the way and to guide professional judgment and behavior.
Competency 2: Engage diversity and difference in practice.
- I promoted conditions within the group settings that encouraged respect for cultural and social diversity among participants.
- The clients served were of diverse socioeconomic statuses and had differences in mental diagnoses than each other. Each client also was of different races, gender, and beliefs.
Competency 3: Advance human rights and social, economic, and environmental justice.
- A significant number of U.S. adults are struggling with mental health issues connected to worry and stress over the novel coronavirus, increasing from 32 percent in March to 53 percent in July (Searing, 2020).
- This project was initiated to address the mental health concerns and needs of attendees of the Lighthouse amidst the COVID-19 Pandemic.
- This project advanced the rights and justices of participants by inspiring them to attend and learn the necessary skills to improve their mental well-being.
Competency 4: Engage In Practice-informed Research and Research-informed Practice
- I engaged in a comprehensive research process of the curriculum that was being utilized by the Lighthouse before the creation of the activities that were utilized in my curriculum.
- Researching evidence-based practices and what has worked for constituents of this population helped me create my curriculum. The research I engaged in helped me improve the delivery of services provided to the Lighthouse constituents.
Competency 5: Engage in Policy Practice
- I reviewed several policies that affect how peer support centers are operated in the state of Tennessee before creating and implementing the curriculum I created.
- One policy involved peer support specialists having to be certified by the state and receive extensive training to be certified before providing direct peer-to-peer support to others who have a mental illness, substance abuse, or co-occurring disorders.
- Another policy involved which topics had to be part of the curriculum to maintain a Certified Peer Support Program status. There is a monthly report provided to the state that reviews all activities that were taught to the Lighthouse participants. I had to ensure my activities met the policy guidelines before creation.
Competency 6: Engage with Individuals, Families, Groups, Organizations, and Communities
- I was able to apply knowledge learned in courses about human behavior and the social environment, person-in-environment, and other multidisciplinary theoretical frameworks, as previously mentioned, to engage with clients and constituencies.
• I utilized empathy, reflection, and interpersonal skills to engage diverse clients and group constituencies effectively. Before beginning each group activity, I would walk around the room and check-in with each participant to see how they had been doing, etc. While engaging with participants, conversations were mentioned about participants’ family members and their relationship with these family members. I also frequently met with my field supervisor and staff members to discuss the group participants’ engagement with the activities I created in the curriculum.
Competency 7: Assess Individuals, Families, Groups, Organizations, and Communities
- Before creating activities for the curriculum, a Pre-Test Survey was conducted to assess areas of interest for each participant of the groups that attended the Lighthouse. This was done at the McNabb Center group homes and other Community-based and privately owned group homes. The results of these surveys were reviewed by myself, the field supervisor, and staff members of the Lighthouse before creating the activities that went into the making of the curriculum.
- I created a Post-Test Survey to assess the effectiveness of the implementation and benefit of the activities I created for the curriculum being used at the Lighthouse currently.
Competency 8: Intervene with Individuals, Families, Groups, Organizations, and Communities
- Interventions were created as activities at a micro-level for individuals, taught to the groups attending, and will be utilized in their home environment and on a community level when interacting in public settings. Interventions took place 2-3 days per week over the course of 2 months.
- The interventions that were chosen set goals for each client to work towards. In many instances, materials were provided for the client to utilize over an extensive amount of time to track their progress on the set goals.
Competency 9: Evaluate Practice with Individuals, Families, Groups, Organizations, and Communities
- Evaluations were conducted before the creation and implementation of the activities created for the curriculum and during the beginning of October to gauge the effectiveness of the interventions discussed in the curriculum activities.
- Evaluations are also being conducted on an on-going basis throughout the curriculum’s duration by the peer support staff of the Lighthouse, which reports back to me regarding if any changes need to be made.
References
Advocates for Human Potential, Inc. (2018). Research findings. Wellness Recovery Action Plan (WRAP) – Your Wellness Your Way. https://mentalhealthrecovery.com/research-findings/
Chinman, M., George, P., Dougherty, R. H., Daniels, A. S., Ghose, S. S., Swift, A., & Delphin-Rittmon, M. E. (2014). Peer support services for individuals with serious mental illnesses: Assessing the evidence. Psychiatric Services, 65(4), 429-441. https://doi.org/10.1176/appi.ps.201300244
Colorado Department of Education. (2020, July 2). Well-being and connection during COVID-19 | CDE. Colorado Department of Education CDE. https://www.cde.state.co.us/safeschools/wellbeing
Cook, J. A., Copeland, M. E., Corey, L., Buffington, E., Jonikas, J. A., Curtis, L. C., Grey, D. D., & Nichols, W. H. (2010). Developing the evidence base for peer-led services: Changes among participants following wellness recovery action planning (WRAP) education in two statewide initiatives. Psychiatric Rehabilitation Journal, 34(2), 113-120. https://doi.org/10.2975/34.2.2010.113.120
Evidence-Based Healthy Aging Program. (, 2020). Review of findings on chronic disease self-management program (CDSMP) outcomes: Physical, emotional & health-related quality of life, healthcare utilization, and costs. Self Management Resources. https://www.selfmanagementresource.com/docs/pdfs/Review_Findings_CDSMP_Outcomes1_8_08.pdf
Fukui, S., Starnino, V. R., Susana, M., Davidson, L. J., Cook, K., Rapp, C. A., & Gowdy, E. A. (2011). Effect of wellness recovery action plan (WRAP) participation on psychiatric symptoms, sense of hope, and recovery. Psychiatric Rehabilitation Journal, 34(3), 214-222. https://doi.org/10.2975/34.3.2011.214.222
Searing, L. (2020, September 4). During a pandemic, the growth of U.S. adults with mental health issues jumps to 53 percent. The Washington Post. https://www.washingtonpost.com/health/covid-worry-stress-mental-health/2020/09/04/609c0dc2-ee03-11ea-99a1-71343d03bc29_story.html
Therapist Aid. (2020). Therapy worksheets, tools, and handouts | Therapist aid. https://www.therapistaid.com