Omni Visions Therapeutic Visitation Training

During my advanced practicum at Omni Visions, I created a Therapeutic Visitation Training Presentation for my special project. Often therapeutic visitation with biological families is court-mandated in the child welfare field if there is a need for therapeutic oversight in addition to supervision. Since Omni Visions is a therapeutic foster care agency that is contracted by the Department of Children Services to meet the needs of higher-level foster cases, Omni Resource Coordinators are obligated to facilitate therapeutic visitation.
I surveyed Omni Resource Coordinators and Team Leaders to find that there was not only a need for further training but that all employees that completed the survey desired additional training on therapeutic visitation. I created and presented an hour-long training that included policies and best practices, research on the background of the families, purpose, and goals of therapeutic visitation. The presentation also included the role and desired qualities of the therapeutic facilitator, as well as effective evidence-based models and practices that can be utilized during the visits. I recorded the presentation and made it available for all 40 Omni Visions of Chattanooga employees. You may view my presentation recording below.
Social Issues
This training presentation focuses on a few social issues. First, it acknowledges that individuals with childhood trauma and high ACE scores are likely to experience poorer outcomes of physical and mental health, poverty, unwanted pregnancies, alcohol and substance abuse, sex trafficking, depression, and many other adverse outcomes in life. Unfortunately, most foster care youth and their biological family members have traumatic pasts and high ACE scores. Another discussion in the presentation is how intergenerational and inherited trauma is prevalent in the foster care field. It is necessary for foster care professionals to understand these issues and backgrounds of the clients, as it will shed light to utilize the person-in-environment perspective.
Another major social issue in the foster care field is how bias professionals tend to be towards biological parents, which can lead to a skewed view and minimal effort towards reunification. I included in the presentation the importance of regular self-assessment of each worker’s biases and ways to better engage and build rapport with each parent. As a contract therapeutic foster care agency, Omni workers are obligated to approach and treat the biological families with the same competence and trauma-informed practice as they do the children. Strengthening the familial bond and promoting resiliency for the family unit should be prioritized. As I noticed how these issues negatively impact the child’s well-being and permanency, as well as the biological family members, I initiated and implemented the therapeutic visitation training as a way to better inform and engage fellow Omni professionals.
Mission

Omni Family of Services advances hope and healing to improve lives, empower people, and strengthen communities. The Therapeutic Visitation Training follows the Omni mission statement and values to uphold emotional intelligence, safety, trustworthiness, embrace diversity, empowerment, and mindful collaboration.
Goals
The primary goal of the training was to provide the Omni workers the knowledge and tools to effectively facilitate therapeutic visitation that will increase the chances of reunification for biological families in the foster care system. The following were the goals of the training presentation:
- Understand the purpose of therapeutic visitation
- Learn common histories and stressors of referred clients
- Become familiar with ACES and how to educate clients on ACES
- Learn policies and best practices of mandated therapeutic visitation
- Identify the role and qualities of an effective facilitator
- Utilize evidence-based interventions during therapeutic visitation
Interventions

- Meet with child and family in a pre-determined safe and appropriate setting
- ACES and Resiliency scales
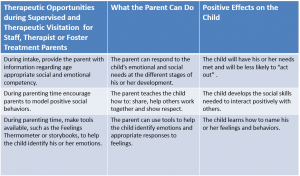
- Teach/Coach parenting skills
- Activities to strengthen the family bond and communication
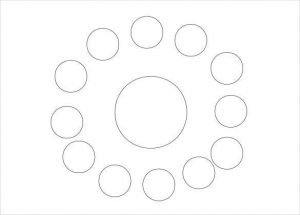
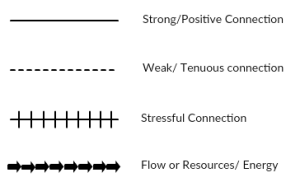
- Ecomap to identify individual and family connections, supports, conflicts, and resiliency factors
- Documentation including DCS Observation Checklist to monitor progress towards reunification
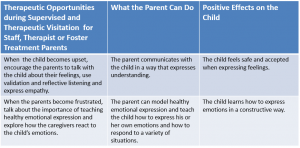
- Teach and monitor emotional identification and regulation
- Participate in all team meetings and testify in court
Therapeutic Interventions that can be used during visitation:
- Motivational Interviewing (MI)
- Parent-Child Interaction Therapy (PCIT)
- Play Therapy Dimensions Model
- Acceptance and Commitment Therapy (ACT)
- Cognitive Behavioral Therapy (CBT)
- Interpersonal Therapy (IPT)
Theoretical Perspectives

The theory that intergenerational transmission of trauma can exist and affect the offspring of parents with trauma should be a foundation of how child welfare workers approach families and reunification. Emerging research shows that children can be affected by parental trauma even if that trauma precedes their birth or conception (Yehuda & Lehrner, 2018). Extreme adverse events and toxic stress can influence a person to such an extent that future generations continue to be impacted in a way that could be described as a post-traumatic state (Yehuda & Lehrner, 2018). Recognizing these potential effects of trauma can help child welfare professionals approach biological families with more compassion while effectively assessing and creating individual and family treatment plans. Measuring ACES, Resiliency Scores, and creating ecomaps may help the facilitator identify the strengths and conflicts of parents and family dynamics before treatment planning.
Dybicz (2015) discusses how the person-in-environment approach, derived from the ecological systems theory, focuses on how heavily a person can be influenced by their environment and experiences. Learning details about a person’s historical and current life experiences may provide an understanding of their behaviors. The therapeutic facilitator will benefit from using this perspective as it will lead to a more holistic awareness of the client(s). Furthermore, the Bowen family systems theory sheds insight into the emotional interdependency of a family, despite disruption in placement or physical proximity (Bowen Center, 2021). It is especially important to recognize this permanent emotional bond when working with families with a chance of reunification.
Parent-Child Interaction Therapy (PCIT) is considered effective with children ages two to seven, but components of the model can also be used when working with children older than seven. Topitzes, Mersky, & McNeil (2015) found that family-inclusive approaches that utilize both individualized treatment plans and coaching were more effective in strengthening the caretaker and child relationship. Various other therapeutic models can be used during the visitation. I only provided a few examples in my training presentation. It is more critical to take time learning all the involved clients and thoroughly assessing before forming a treatment plan, so the facilitator can utilize the most effective evidence-based interventions that match the client(s) and situation. Motivational interviewing is helpful for child welfare workers to use to help ambivalent clients consider their willingness to change and improve their life situations (Child Welfare Information Gateway, 2017).
Bowen Center. (2021). Introduction to the eight concepts. https://www.thebowencenter.org/introduction-eight-concepts
Child Welfare Information Gateway. (2017, December). Motivational interviewing: A primer for child welfare professionals [Fact Sheet]. U.S. Department of Health and Human Services, Children’s Bureau. https://www.childwelfare.gov/pubPDFs/motivational_interviewing.pdf
Dybicz, P. (2015, April). From person-in-environment to strengths: The promise of postmodern practice. Journal of Social Work Education, 51(2), 237-249. https://www.researchgate.net/publication/283865105_From_Person-in-Environment_to_Strengths_The_Promise_of_Postmodern_Practice
Topitzes, Mersky, & McNeil (2015, January). Implementation of parent child interaction therapy within foster care: An attempt to translate an evidence-based program within a local child welfare agency. Journal of Public Child Welfare, 9(1), 22-41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4342056/
Yehuda, R. & Lehrner, A. (2018). Intergenerational transmission of trauma effects: Putative role of epigenetic mechanisms. World Psychiatry, 17(3), 243–257. https://doi.org/10.1002/wps.20568
Results
The training’s target population focused on foster children and their biological families. While these families are the primary population concerning therapeutic visitation, the Omni Resource Coordinators also benefited from the training’s information. I created a post-test that included rating the training and testing for knowledge on therapeutic visitation. These post-tests showed that all employees felt the training was beneficial and increased their therapeutic skills. Many Omni employees praised my training presentation and showed appreciation for me taking the time to help employees understand more effective practices when interacting with families. DCS and Omni Visions evaluate the number of reunification cases each quarter and annually. These future evaluations will show a clearer result if the training had any long-lasting impact on the reunification of families.
Conclusions
This therapeutic visitation training gave me the opportunity to learn evidence-based interventions effective in strengthening familial bonds and increasing chances of reunification. I also learned policies and the importance of documentation and communication with all parties involved on the child’s team. An unexpected result of my special project was understanding discrimination often experienced by biological family members during the reunification process and how this discrimination can actually negatively impact the biological family member to the extent that they do not actively participate in completing their permanency plan. These factors also negatively impact the number of successful reunifications in the child welfare system.
There were some limitations to this training. Due to the COVID-19 pandemic, the agency was limiting in-person gatherings. This meant that I had to record my presentation and distribute it to employees via email. Since the training was not on a scheduled date and in-person, all employees have till September 2021 to complete it. The extended date is also due to a string of audits occurring from Spring to early Summer. This date will be after my practicum is complete. Fortunately, I have transitioned into a therapist role within the agency which allows me to still review the evaluation surveys of the employees that had not yet completed the training during my practicum.
I would have preferred the training to be in person because one way it could have been more effective would have been if employees could have gathered in small groups to complete some activities. These activities include completing an ecomap, ACE questionnaire, and practice motivational interviewing and hypothetical situations of offering interventions for the family. I would have liked to give employees various scenarios that warrant interventions and practical parenting coaching. Since I will remain at Omni as a Level 3 Therapist, I hope to have future opportunities to not only improve this training curriculum but also present in-person to small groups.
Competencies

Competency 1: Ethics and Professionalism
- The therapeutic visitation training provides a practice framework for foster care professionals that reflects a commitment to the values and ethics of the social work field. The NASW Code of Ethics for Child Welfare Workers is present throughout the presentation.
- Biological family members should be treated fairly and fully supported during the reunification process.
- The training provides continuing education while promoting ongoing consultation while facilitating therapeutic visitation.
- Therapeutic facilitators must present themselves professionally at all times when working with families.
- I demonstrated professional oral and written skills by creating and presenting the training curriculum.
Competency 2: Diversity
- The training utilizes the person-in-environment perspective to allow for facilitators to learn the historical and current stressors of each biological family member and foster child.
- Facilitators need to understand common backgrounds of families include high ACE scores, domestic violence, poverty, trauma, mental health issues, substance abuse, neglect, and abuse. Self-assessment of the professional is essential to avoid personal biases.
- Cultural competency is key when working with families. The training discusses how professionals must have the ability to respond respectfully to people of all cultures, classes, races, sexual orientations, religions, and ethnic backgrounds while affirming and valuing the worth of all individuals and families. It is also helpful to learn cultural values that may influence parenting techniques and family dynamics.
Competency 3: Human Rights and Justice
- The training promotes social justice for biological families. Biological family members should receive supportive services and resources to promote stability and reunification. Ongoing bias towards biological family members is an issue often present in the foster care field. This issue deserves advocacy and attention as it negatively affects foster youth and family preservation.
- The therapeutic visitation facilitator should include all members of the child and family team in regular communication. This includes the biological family member’s legal representation, as well as the child’s guardian ad litem to ensure that all parties are legally represented throughout the reunification process.
Competency 4: Research
- The training includes evidence-based practices that are found effective to strengthen familial bonds, stability, communication, and emotional stability. It is imperative that therapeutic visitation focus on healing from past family conflict cycles. Cognitive-behavioral therapy, Parent-Child Interaction Therapy, Bowen Family Systems Theory, Interpersonal Therapy, and Acceptance and Commitment Therapy are all models that should be reviewed and utilized by the facilitator.
- I personally conducted research through surveys among Omni Visions professionals and learned there was a need for therapeutic visitation training. All Omni Resource Coordinators and Team Leaders that completed the surveys responded that they feel further training on therapeutic visitation was needed within the agency.
Competency 5: Policy
- The training covered policies concerning court-mandated therapeutic visitation in foster care. A bachelor’s level facilitator must be directly supervised by a Master’s level clinician. Proper documentation including detailed session notes and the DCS Observation Checklist form should be completed within 48 hours of each visit.
- DCS policy states that each biological family member will be provided a permanency plan that includes all steps that need to be complete before reunification. This permanency plan should be monitored during the process of visits. Family members will need proper assistance from the team while completing each step on the permanency plan. This permanency plan deserves attention as DCS has the power to file for termination of parental rights after the child has been in foster care for six months or longer.
- I met with Omni Visions’ upper management and advocated for an additional policy to be enforced for all therapeutic visitation. This policy would require the child’s therapist to be present for the first three visitation sessions and then once a month for all future sessions.
Competency 6: Engagement
- I spent a substantial amount of time reviewing the evidence-based practices and strategies mentioned under Competency four that would be effective during therapeutic visitation. Motivational Interviewing specific to child welfare professionals was also a main focus during the presentation to promote engagement with families.
- I emphasized the importance of the engagement process, as it is necessary for the biological family members and children to feel safe and supported during the visits. Consideration of the historical background and current stressors of each member is critical for such engagement to occur.
- The role and qualities of an effective facilitator will also affect the engagement process. The facilitator must present themselves as caring, objective, culturally competent, ethical, open-minded, and warm to achieve therapeutic engagement. Ensuring neutrality, regular communication, and constructive feedback and re-direction are all a part of engaging the clients on an individual level, as well as a family unit.
Competency 7: Assessment
- Various assessment tools are helpful during therapeutic visitation. Assessing ACES and resiliency can help the facilitator better understand each family member and create SMART goals for a treatment plan. The ACES questionnaire, The Child and Youth Resiliency Measure (CYRM), and The Resiliency Scale for Adults are included as training materials. I also recommended completing an ecomap for each child and family member as a visual aid to understanding strengths, conflicting factors, and social supports. An ecomap template was included in the training materials. I encouraged facilitators to complete these assessments for each family member during the initial sessions.
- Assessing for emotional and physical safety is also included in the training. This should be done before, during, and after each visitation session.
- The DCS Observation Checklist and detailed case notes should also be completed within 48 hours. Regular communication with the child and family team will help keep everyone updated on progress. The permanency plan should be regularly assessed with progress so that goals and treatment plans can be readjusted to continue the momentum towards reunification.



Competency 8: Intervention
- The training teaches how the facilitator can use Motivational Interviewing, Cognitive-Behavioral Therapy, Parent-Child Interaction Therapy, Bowen Family Systems Theory, Interpersonal Therapy, Play Therapy Dimensions Model, and Acceptance and Commitment Therapy during therapeutic visitation sessions to help repair conflict cycles, strengthen family dynamics, promote resiliency, and teach parenting skills.
- During each therapeutic visitation session, the facilitator has the opportunity to teach the parent appropriate parenting interventions. The training provided some examples of such interventions.
- I recommended that facilitators receive regular supervision from Masters level superiors while providing therapeutic services to the families. I was also able to use my own learned knowledge from this special project as I provided effective interventions during therapeutic supervision with biological families.
- The facilitator should also ensure that each biological family member and child are receiving individual resources that may be needed to work towards reunification. Child and Family Team Meetings (CFTM) should occur regularly to assess and discuss progress towards reunification. These meetings need to include all child welfare professionals, legal representation, the child, and biological family members included in the permanency plan.
Competency 9: Evaluation
- I created an evaluation survey for all participants to complete after receiving the training. The survey included post-test questions as well as an evaluation of the presenter and training.
- Continuous evaluation of progress towards reunification should occur during the CFTMs. The facilitator should keep detailed documentation and communicate progress to all members of the child’s team.
- I requested meetings for my field instructor to evaluate my special project training throughout the semester of practicum. My field instructor was also able to evaluate the final presentation. I received positive reviews that the training was beneficial and would be utilized to continuously train Resource Coordinators on therapeutic visitation.